
History:
Brianna presented to the cardiology department for a loud heart murmur which was found on her first puppy visits. She was clinically doing well at home, with no cardiac or respiratory changes noted by the owner.
Cardiac Physical Exam:
HR: 190 RR: 30 Wt: 2.0kg
MM: Pink, CRT <2
H/L: Grade V/VI continuous murmur, PMI left base. Sinus tachycardia. Jugular at the bottom of the neck.
Pulses: Bounding pulses. Synchronous with the heartbeat.
Echocardiographic highlights:
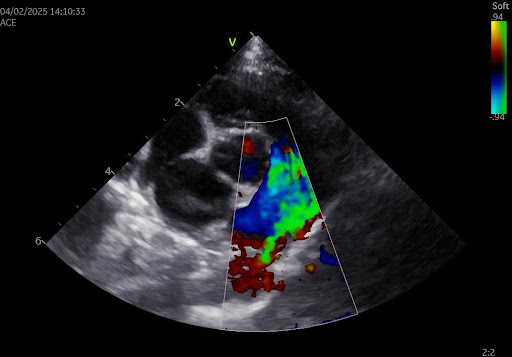
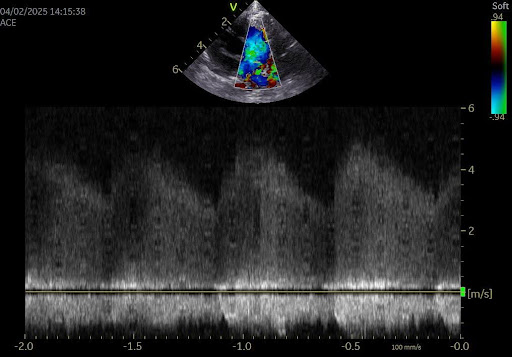
The left atrium is mildly enlarged. The left ventricular walls are normal in thickness with a moderately dilated LV cavity and normal contractile function. The mitral valve is subjectively normal in appearance. The right heart is normal in size. There is continuous flow left to right flow (4.7 m/s) entering the pulmonary artery. The main PA and the PA branches are mildly enlarged. No B lines seen, no pleural or pericardial effusion present.
Diagnosis:
Left to right shunting patent ductus arteriosus with mild to moderate left sided cardiac enlargement
Treatment options:
Surgical Ligation: This approach involves an open chest procedure (thoracotomy), during which the surgeon will manually tie off the abnormal blood vessel using suture. This approach is often necessary in patients who are small in size, and whose femoral artery cannot accommodate the catheter necessary for a minimally invasive approach.
Minimally Invasive Approach:
This technique involves making a small incision on the thigh to access the femoral artery. A long catheter is then passed through the femoral artery, and used to deploy a device (typically an ACDO – Amplatz Canine Ductal Occluder) within the ductus. This device occludes the ductus and stops the abnormal flow of blood. Traditionally this procedure was not possible in patients as small as Brianna due to the size of the required catheter and introducer. However, with the introduction of a newer device called an AVP-4 (Amplatzer Vascular Plug 4), which uses a smaller catheter size, we are now able to accommodate smaller patients. That being said Brianna was still on the small side even for this device. After considering the options Brianna’s owners elected a surgical approach.
Surgery:
Brianna presented to the surgery department for her PDA ligation with Dr. Jacob Rubin. Her surgery went well and she recovered uneventfully. The following morning there was no murmur heard, and Brianna’s incision was comfortable. She was discharged that day with the plan to follow up in 2-3 months.
Recheck:
Brianna recently presented to the cardiology department for her recheck exam. Her recheck echocardiogram did not reveal any residual flow through the ductus, and the cardiac chambers and function were normal. Brianna is now considered to be essentially normal patient from a cardiac standpoint, and does not require any long term cardiac medications or follow up. Her case highlights the excellent collaboration between the referring community, who identified this murmur early, and the multiple specialties involved in managing these cases.